
.jpg?width=862&height=513&name=Laudio-Insights---Charts---RN-Turnover-by-month%20(1).jpg)
What the data says
The dark blue line represents the average RN annualized monthly turnover rate for the last 12 months. The calculation is in Full Time Equivalents (FTEs); in other words, part-time and per diem employees have less impact than full-time employees.
The dotted line represents the average RN annualized monthly turnover rate for the year prior. Given the seasonality of turnover, comparing same period turnover rates from one year to the next helps clarify trends in turnover.
The last 12 months average 16.2% RN turnover, relative to 18.9% a year earlier.
Such an improvement in RN turnover will have saved a typical 500-bed hospital (e.g., with 1,000 RN FTEs) 27 RN terminations annually, equal to ~$1.4M in annual savings, based on average turnover costs (see footnote). This observed improvement in retention will also have positive impacts on team culture, well-being, and predictable coverage of gaps in shifts.
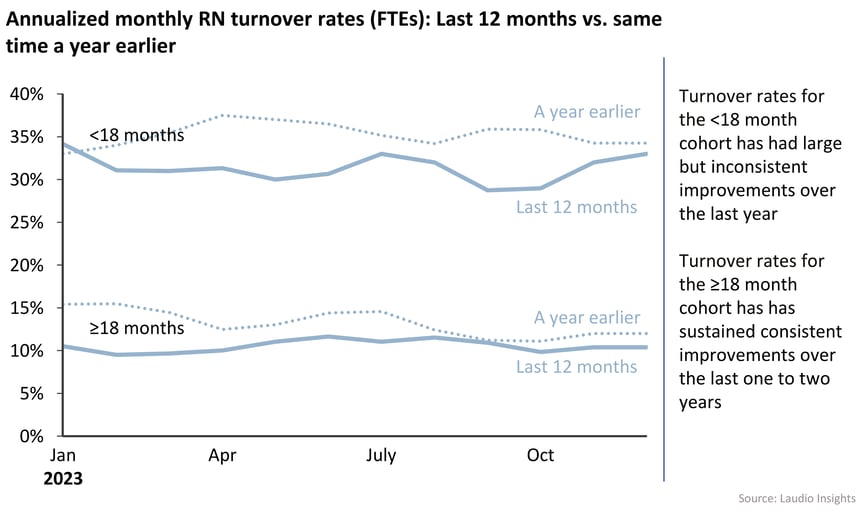
The second chart shows RN turnover trends disaggregated into two segments: RNs with 18 months or less of tenure and RNs with 18 months or more.
For employees with up to 18 months tenure, the YoY trend has improved over the last year but inconsistently (see the top two lines in the graph below).
When looking at the same chart for RNs with 18 months or more of tenure, turnover has been flat the last 12 months, turnover has improved and those improvements have been consistently sustained over the last 12 months (see the bottom two lines in the graph below).
What it means
1 - The “Great Resignation” is behind us: the gains seen over the last couple of years have mostly been from a “return to normalcy” in later-tenure employees.
-
- During the acute COVID era (i.e., late 2021 and early 2022), turnover rates for higher-tenured RNs were at an all-time high. The “Great Resignation” and early retirements during that time sent the typically more stable cohort of higher-tenure RNs into higher turnover rates typically only seen in very early tenure cohorts. The large decline and sustained improvement over the past two years indicates that era is behind us, and higher-tenure turnover has returned to historical norms.
2 - A perceived lack of growth opportunities remains a main cause for persistently elevated early-tenure turnover.
-
- This improvement in retention doesn’t necessarily mean that underlying challenges in turnover have been resolved.
- While employees with the greatest tenures are staying with their organizations at levels closer to historical norms, the challenges of higher turnover remain for early-tenure team members. According to one COO:
“Employees tend to leave after a year for a role at another organization to get into a specialty or get a better schedule or a better salary. They rarely see the same level of opportunities in the organization that they are in.”
What the implications are for healthcare leaders
1 - To maintain the momentum of improvements in turnover, which have been mostly systemic in the past few years, health systems need to implement tools and practices that have been proven to have an impact.
-
- Health systems should consider implementing new hire check-ins at multiple points in the employees’ first year, to provide easy-to-use tools to complete and document them, and to build a discussion of how the manager is doing with them in 1-1 meetings with their directors. New Hire check-ins are an impactful mechanism to continue to improve early-tenure retention. (Proof of the outsized impact that these activities have will appear in an upcoming article.) Different questions can be scripted for 30-day vs. 90-day vs. 6-month milestones to help them be most mutually beneficial.
- Health systems should consider implementing a system where managers are having monthly meaningful interactions with each team member. (Proof of these activities' outsized impact will appear in an upcoming article.) These include stay interviews, recognition of real work done, and checking in on professional development goals.
2 - To address the perceived lack of growth opportunities for new employees and impact persistent early tenure turnover, health systems need to create equal growth opportunities for those who stay as are available to those who leave.
-
- Make it part of the plan for employees to move between departments.
- Managers can benefit from developing an “attitude of generativity”: that they are developing employees for the greater organization, not just their own department. Most leaders today experience a sense of loss and frustration as employees move to different units in the organization but in moderation, managers who are effective at finding new homes internally are improving retention rates.
- Executives should celebrate managers who are effective at finding employees their next homes; they are avoiding the employee leaving for another organization. Difficult as it may be, managers should be encouraged by their leaders to welcome and support team members who ask to switch to another area.
- Health systems that create and make such opportunities visible to their employees will be more successful in retaining them, especially in competitive markets. “The way you increase your salary and progress your career more quickly is to jump from one organization to another,” observed one health system VP in a recent conversation about this topic. Ideally, well-performing employees should have similar opportunities for forward progression within their organization as they can find elsewhere.
- Implement professional pathways (e.g., clinical ladders); these are another way to create growth opportunities within an organization.
- All leaders, both clinical and non-clinical, should consider implementing professional pathways for team members directly tied to specific and progressive competencies (e.g., clinical ladders can be one such example); those who have such programs should consider increasing the number of steps in those programs, as long as the steps are meaningful. Programs with more steps provide more growth opportunities with each role.
- Executives should consider building new pathways for growth within their organization and advertising them at internal career fairs. While there are complications around implementing such an approach - such as acknowledging that it takes time to change entrenched perspectives amongst the leadership team for such an adjustment - note that frontline employees have already made the change in perspective.
- Make it part of the plan for employees to move between departments.
Areas for future analysis and discussion
-
- How has early tenure retention trended over a longer period of time - e.g., the last four years?
- What is the isolated impact of new hire check-ins on early tenure retention?
Data definition
- Turnover calculation:
- FTEs who resigned, retired, expired, or were terminated in a given month, divided by the total FTEs employed at any point during the month.
- Exclusion criteria:
- Departmental transfers within the same facility are not included as terminations.
- Employees who reduce hours (e.g., who go from FT to PT) are not included as terminations.
- Transfers between facilities within a health system are not counted.
- Any employee terminated on the same day as their hire date are not counted.
- Inclusion criteria:
- The manager of the department is included in the numerator and denominator.
- Any employee who was terminated and/or hired at any point in the month is considered as having worked for the complete month.
- Any employee who transfers department at any point in the month is considered as having worked only in the new department (not the one they transferred out of) for that complete month.
Footnote
- One published average cost of turnover for a staff RN is “$52,350, with the range averaging $40,200 to $64,500” per the 2023 NSI National Health Care Retention & RN Staffing Report. Health systems in competitive urban markets could have substantially higher costs.