
What the data says
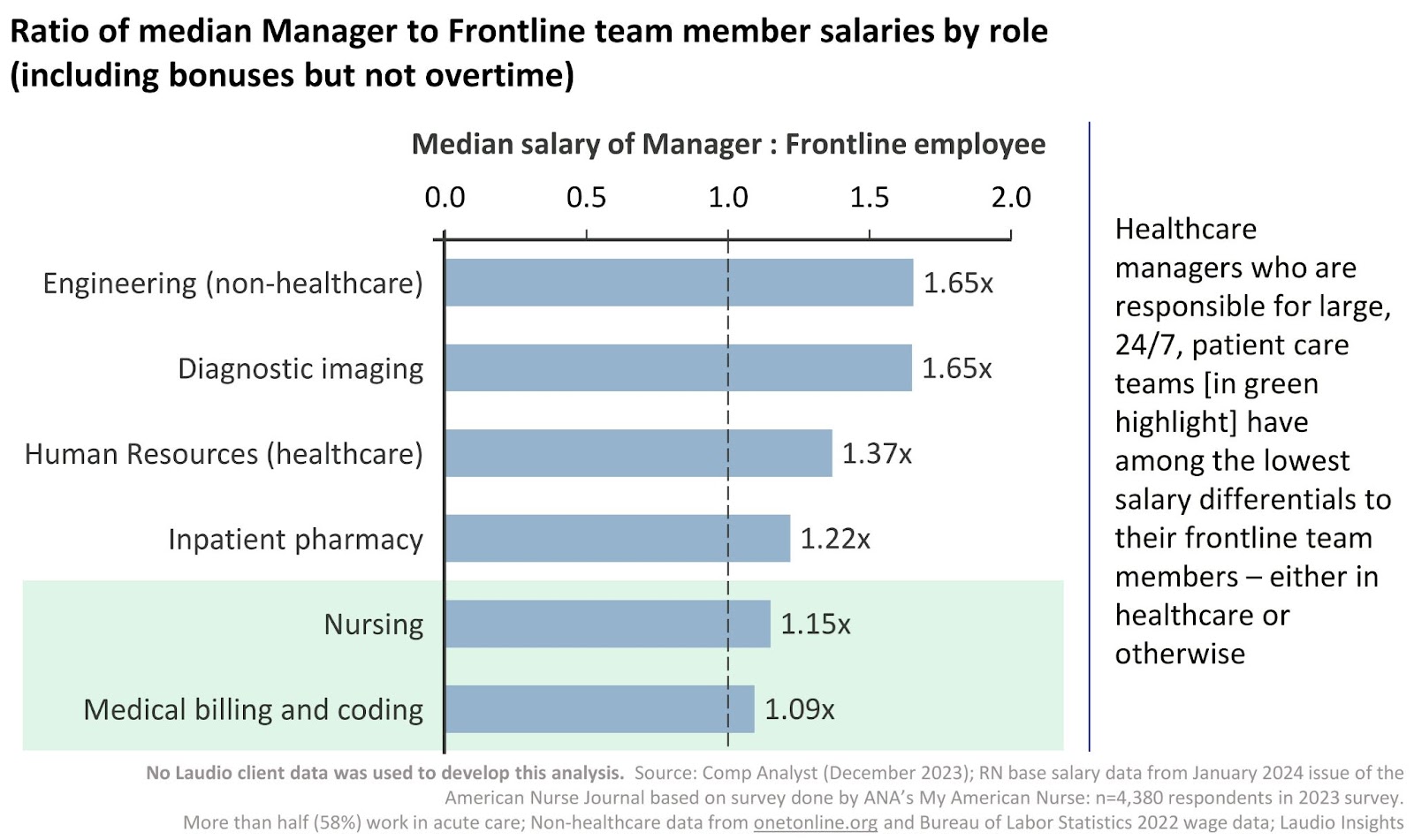
Median nurse manager salaries are about 15% higher than the median RN salary (all salaries shown are total cash compensation, not including overtime, for which frontline RNs typically have adequate opportunity to sign up). Inpatient pharmacy managers average 22% higher salaries.
Also within health systems, HR managers average 37% higher salaries than HR business partners and diagnostic imaging managers average 65% higher salaries than imaging technicians (it should be noted that imaging managers often have a BS or higher degree while imaging technicians often do not, which explains some of the larger gap).
Outside of healthcare, the engineering manager to frontline employee ratio, for example, averages 1.65x. At the same time, in non-healthcare industries, the average manager’s span of control is around four or five employees. Nurse managers lead 40 or more frontline team members on average – this is a level of leadership that would better equate them to VPs or above outside of healthcare.
What it means
Nurse manager salary levels, in particular, are rooted in an outdated vision of the role.
The 15% pay differential for nurse managers reflects the historical nature of the role rather than the responsibilities of the role today. There is a gap between the perception and on-the-ground reality of the nurse manager role; the salary difference is one symptom of that.
-
- The nurse manager salary difference does not reflect the major responsibilities of the managers (especially those with high acuity, 24/7, and/or large spans of control teams), the time and pressure of the job of frontline healthcare leadership, or the outsized role that these managers have in achieving organizational outcomes.
- The difference exists because salaries are not directly synced with managers’ individual impact on organizational outcomes.
- In many organizations, nursing is considered a cost center, whereas pharmacy, for example, is considered a profit or revenue center. This may explain some of the historical gap; however, nurse managers have as much potential to influence major cost and quality/reputation outcomes.
If health systems do not address the salary issue, fewer RNs may want to become managers, which will continue to perpetuate critical levels of leadership scarcity.
-
- Many health systems are already struggling to build a pipeline of qualified and interested internal candidates for manager roles; this is at least partly due to the lack of clear incentives to offset the heavy burdens that accompany management positions.
- In some cases, union rules also exacerbate the scarcity (e.g., once RNs transition to a leadership role, they cannot return to staff nursing).
As tight margins are pushing health systems to try to do more with less, the level of investment in managers could potentially decrease – unless there is an ROI-based business case to increase it.
- There are many examples in academic literature showing that the impact of effective nurse leaders is significantly correlated with higher nursing retention rates (e.g., Lee, 2023), a mounting challenge for health systems nationwide.
- Other research shows the significant impact managers can have on patient safety. For example, a patient fall with injury is estimated to cost a hospital about $14,000 (Dykes et al., 2023). Evidence indicates that effective nurse leaders who set clear expectations and support fall policy adherence improve fall outcomes (Turner et al., 2020).
What the implications are for healthcare leaders
Executives can benefit from a deeper understanding of the nurse manager role and the impact that high-performing frontline leaders can have on their organization’s outcomes.
- Most health system executives agree with the phrase “the nurse manager has the hardest job in the hospital.” While true, perhaps a more forward-looking version of the phrase might be that “the nurse manager is the role with the greatest impact on our financial, quality, and team engagement outcomes.”
- The former phrase imparts much-needed empathy for the leaders; the second imparts a greater understanding of the strategic and financial investments required to fully enlist managers in optimizing all the opportunities of organizational outcomes.
- The low salaries and outdated perspective are anchored in the historical role of the “head nurse” – a role more akin to a charge nurse today. In the last twenty years, the nurse manager role has become one of the most complex (managing high acuity, 24/7, and/or large spans of control teams) and one of the greatest leverage points for organizational outcomes, similar to the president of a critical business unit.
- Nurse managers own the outcomes of patient safety, patient experience, employee engagement scores, and retention while maintaining all the responsibilities of team leadership, onboarding, staffing, scheduling processes, and financial performance.
Increasing the pay differential could boost interest from the highest-performing team members to meet future leadership needs.
- While being a frontline RN is a physically and mentally demanding job, it is time-bounded; RNs often work three twelve-hour days a week, with limited phone call/on-call/after-hours requirements. RNs are often able to pick up extra shifts and are paid overtime for doing so.
- In comparison, nurse managers often work five ten-hour days while being on-call and available to support and problem-solve around-the-clock, with no possibility of overtime pay. When frontline RNs see their exhausted, overburdened managers, their aspirations for promotion to a manager role are limited. Higher compensation may increase that desire.
- While other benefits, such as offering “work from home” days or providing new/additional administrative support, should also be on the table, their applicability can vary depending on the needs of the department and broader organization.
A business case for updated compensation approaches for nurse managers are essential in order to make them partners in the value that they create. One key way health systems can better align nurse manager pay with their impact is through the use of manager-specific bonuses.
- Given all of the actions and responsibilities of the nurse manager, executives can consider updated incentive plans that provide bonuses when they reach certain targeted outcomes with their teams. The incentive plan could be 20-30% of their base salary, in order to bring their manager compensation in line with other national averages, such as non-clinical areas in health systems.
- Many organizations have bonuses (of around 10%) tied to overall performance goals; the incentive plan can maintain this component as needed, but the amount is not sufficient.
- An additional 10-20% bonus attached specifically to individual department metrics that the managers can wholly influence would offer pay more commensurate with impact.
- Many frontline managers have been disempowered from optimizing incentive-based outcomes, so new communication will be needed to help them to understand their impact and to encourage their leadership in maximizing those metrics.
- A bonus could be created focused on YoY RN turnover of the overall service line. While turnover for an individual department might be too variable to compare year over year, a comparison of average turnover across several departments is possible. If ten Med Surg units have an average RN turnover rate of 18% this year, why not provide bonuses for all managers if the overall average is 17% or lower next year?
- A similar bonus could be created for employee engagement scores or NDNQI® scores (especially the PES-NWI), where the manager has the most direct influence; patient experience, early-tenure turnover, or quality and safety metrics could also be part of the program.
- The manager is the most valuable stakeholder in identifying the root cause of any immediate challenges and addressing them quickly, while also being the greatest leverage point for achieving new opportunities. To offer them such an incentive plan is to directly align them with organizational priorities and underscore that they are critical partners in the next phase of an organizations’ growth. It could also go a long way in inspiring the next generation of leaders.
Sources
- No Laudio client data was used to develop this analysis.
- Source for nurse salary data: American Nurse Journal (January 2024 issue) based on survey done by ANA’s My American Nurse; n=4,380 respondents in 2023 survey: https://www.myamericannurse.com/trends-and-salary-results/
- Source for non-nurse salary data from Comp Analyst (December 2023)
- Source for non-healthcare salary data from onetonline.org and Bureau of Labor Statistics 2022 wage data.
- Dykes, P. C., Curtin-Bowen, M., Lipsitz, S., Franz, C., Adelman, J., Adkison, L., Bogaisky, M., Carroll, D., Carter, E., Herlihy, L., Lindros, M. E., Ryan, V., Scanlan, M., Walsh, M. A., Wien, M., & Bates, D. W. (2023). Cost of inpatient falls and cost-benefit analysis of implementation of an evidence-based fall prevention program. JAMA Health Forum, 4(1), e225125. https://doi.org/10.1001/jamahealthforum.2022.5125
- Lee, S. E., Hyunjie, L., & Sang, S. (2023). Nurse managers’ leadership, patient safety, and quality of care: A systematic review. Western Journal of Nursing Research, 45(2), 176–185. https://doi.org/10.1177/01939459221114079
- Turner, K., Staggs, V., Potter, C., Cramer, E., Shorr, R., Mion, L.C. (2020). Fall prevention implementation strategies in use at 60 United States hospitals: a descriptive study. BMJ Quality & Safety, 29(12), 1000-1007. https://doi.org/10.1136/bmjqs-2019-010642